Fill Out a Valid Alabama 369 Form
Fill Out a Valid Alabama 369 Form
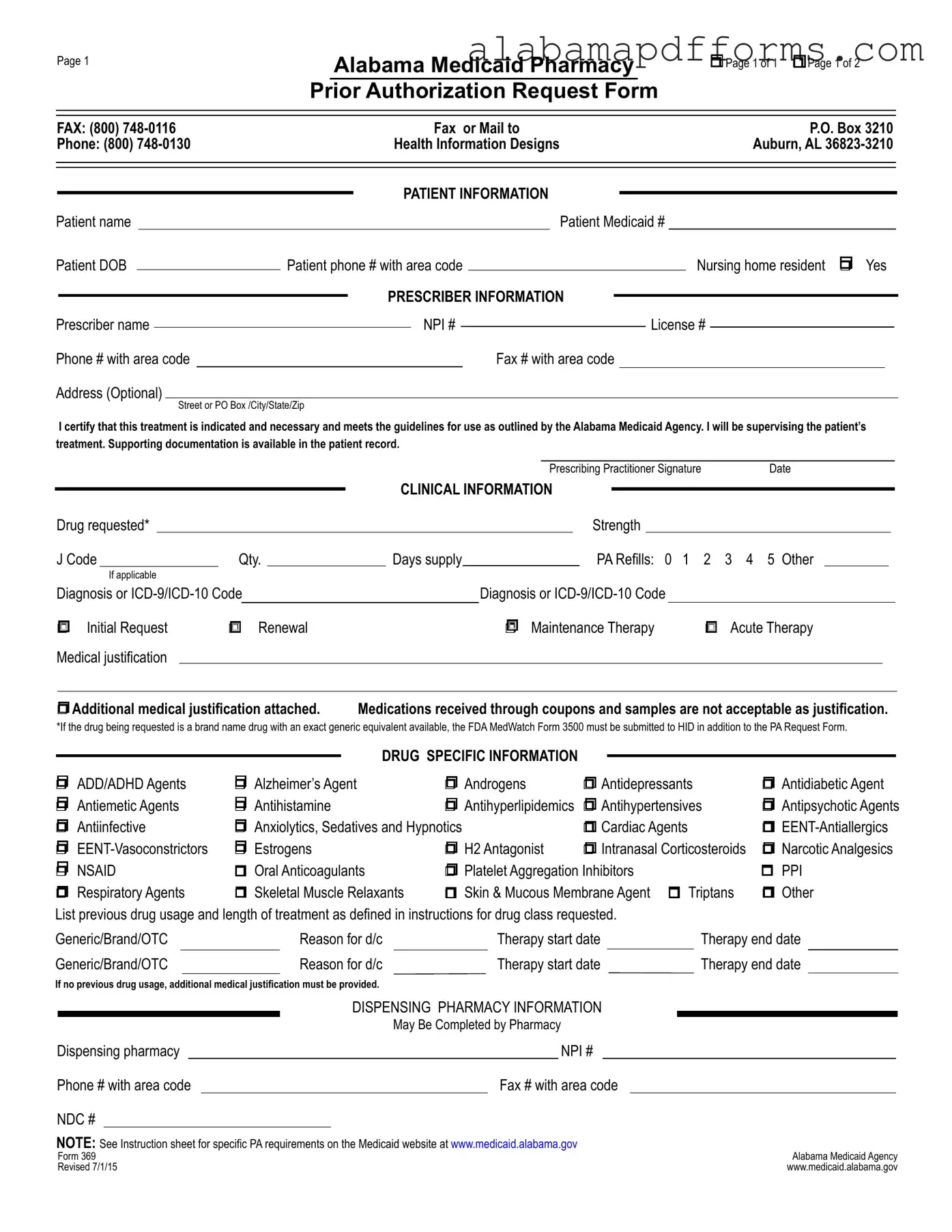
The Alabama 369 form is a critical document used for the prior authorization of pharmacy services under the Alabama Medicaid program. This form facilitates the approval process for specific medications, ensuring that patients receive necessary treatments while adhering to Medicaid guidelines. It collects essential information, including patient and prescriber details, clinical information about the requested drug, and medical justification for its use. The form also requires the prescriber to certify that the treatment is appropriate and necessary, which helps maintain the integrity of patient care. Additionally, the Alabama 369 form outlines specific requirements for various drug classes, such as ADHD agents, antidepressants, and antipsychotics, among others. It also addresses the need for supporting documentation and previous treatment history, which are crucial for evaluating the request. By streamlining the authorization process, the Alabama 369 form plays a vital role in ensuring that patients have access to the medications they need while also preventing misuse and ensuring compliance with established medical standards.
Misconceptions about the Alabama 369 form can lead to confusion and errors in the prior authorization process. Here are ten common misconceptions, along with clarifications.
Understanding these misconceptions can help ensure the proper use of the Alabama 369 form and facilitate a smoother prior authorization process.

Page 1
Alabama Medicaid Pharmacy
Prior Authorization Request Form
rPage 1 of 1 r Page 1 of 2
FAX: (800) |
|
|
|
Fax or Mail to |
|
|
|
|
P.O. Box 3210 |
|
|||||||||||||
Phone: (800) |
|
|
Health Information Designs |
|
|
|
|
Auburn, AL |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Patient name |
|
|
|
|
|
|
|
|
Patient Medicaid # |
|
|
||||||||||||
Patient DOB |
|
|
Patient phone # with area code |
|
|
|
|
Nursing home resident r Yes |
|
||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
PRESCRIBER INFORMATION |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Prescriber name |
|
|
|
|
|
|
NPI # |
|
|
|
|
License # |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Phone # with area code |
|
|
|
|
|
|
Fax # with area code |
|
|
|
|
|
|
|
|
||||||||
Address (Optional) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
I certify that this treatment is indicated and necessary and meets the guidelines for use as outlined by the Alabama Medicaid Agency. I will be supervising the patient’s treatment. Supporting documentation is available in the patient record.
|
|
|
|
|
|
|
|
|
|
|
|
|
Prescribing Practitioner Signature |
Date |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Drug requested* |
|
|
|
|
|
|
|
|
|
|
|
Strength |
|
|
|
|
|
|
|
||||
|
J Code |
Qty. |
|
Days supply |
|
|
|
PA Refills: 0 1 |
2 3 4 5 Other |
|
||||||||||||||
|
|
If applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Diagnosis or |
|
|
|
Diagnosis or |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
r Initial Request |
r Renewal |
|
|
|
r |
Maintenance Therapy |
r Acute Therapy |
|
|||||||||||||||
|
Medical justification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
r Additional medical justification attached. |
Medications received through coupons and samples are not acceptable as justification. |
|
|||||||||||||||||||||
*If the drug being requested is a brand name drug with an exact generic equivalent available, the FDA MedWatch Form 3500 must be submitted to HID in addition to the PA Request Form.
|
|
|
|
|
|
|
|
|
|
DRUG SPECIFIC INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
||
r ADD/ADHD Agents |
r Alzheimer’s Agent |
r Androgens |
r Antidepressants |
r Antidiabetic Agent |
|||
r Antiemetic Agents |
r Antihistamine |
r Antihyperlipidemics |
r Antihypertensives |
r Antipsychotic Agents |
|||
r Antiinfective |
r Anxiolytics, Sedatives and Hypnotics |
r Cardiac Agents |
r |
||||
r |
r Estrogens |
r H2 Antagonist |
r Intranasal Corticosteroids |
r Narcotic Analgesics |
|||
r NSAID |
r Oral Anticoagulants |
r Platelet Aggregation Inhibitors |
r PPI |
||||
r Respiratory Agents |
r Skeletal Muscle Relaxants |
r Skin & Mucous Membrane Agent r Triptans |
r Other |
||||
List previous drug usage and length of treatment as defined in instructions for drug class requested. |
|
|
|
|
||||||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
|
Therapy end date |
|
||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
Therapy end date |
|
|||||||||||
If no previous drug usage, additional medical justification must be provided. |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISPENSING PHARMACY INFORMATION |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
May Be Completed by Pharmacy |
|
|
|
|
|||||
Dispensing pharmacy |
|
|
|
|
|
NPI # |
|
|
|
|
|
|||||||
Phone # with area code |
|
|
|
|
Fax # with area code |
|
|
|
|
|
||||||||
NDC # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
NOTE: See Instruction sheet for specific PA requirements on the Medicaid website at www.medicaid.alabama.gov |
|
Alabama Medicaid Agency |
||||||||||||||||
Form 369 |
|
|
|
|
|
|
|
|
|
|||||||||
Revised 7/1/15 |
|
|
|
|
|
|
|
|
|
www.medicaid.alabama.gov |
||||||||
Page 2 |
Patient Medicaid # |
rSustained Release Oral Opioid Agonist
Proposed duration of therapy |
|
|
|
|
Is medicine for PRN use? |
r Yes |
r No |
|
|||
Type of pain r Acute r Chronic |
|
|
|
Severity of pain: r Mild |
r Moderate r Severe |
|
|||||
Is there a history of substance abuse or addiction? r Yes |
r No |
|
|
|
|||||||
If yes, is treatment plan attached? |
r Yes r No |
|
|
|
|
|
|
|
|
||
Indicate prior and/or current analgesic therapy and alternative management choices |
|
|
|
||||||||
Drug/therapy |
|
|
|
|
Reason for d/c |
|
|
|
|
|
|
Drug/therapy |
|
|
|
Reason for d/c |
|
|
|
|
|||
|
|
|
|
|
|||||||
r Antipsychotic Agents |
The request is for: |
r Monotherapy or r Polytherapy |
|
|
|||||||
For children < 6 years of age, have monitoring protocols (see Attachment C on the Alabama Medicaid website) been followed? r Yes r No For polytherapy and/or
Medical justification may include peer reviewed literature, medical record documentation, chart notes with specific symptoms that the support the diagnosis, etc.
rXenicalR
r |
If initial request |
Weight |
|
kg. |
|
Height |
|
inches |
BMI |
|
|
kg/m2 |
|||
r |
If renewal request |
Previous weight |
|
|
|
kg. |
Current weight |
|
|
|
kg. |
|
|
||
Documentation MD supervised exercise/diet regimen > 6 mo.? r Yes |
r No |
Planned adjunctive therapy? r Yes |
r No |
||||||||||||
r Phosphodiesterase Inhibitors |
|
|
|
|
|
|
|
|
||
Failure or inadequate response to the following alternate therapies: |
|
|
|
|
|
|||||
1. |
|
|
|
2. |
|
|
3. |
|
|
|
4. |
|
|
|
5. |
|
|
6. |
|
|
|
Contraindication of alternate therapies: |
|
|
|
|
|
|
|
|
||
r Documentation of vasoreactivity test attached |
r Consultation with specialist attached |
|
|
|||||||
|
|
|
|
|
|
|||||
r Specialized Nutritionals |
Height |
inches |
Current weight |
kg. |
|
|||||
rIf < 21 years of age, record supports that > 50% of need is met by specialized nutrition
rIf > 21 years of age, record supports 100% of need is met by specialized nutrition
Method of administration |
|
Duration |
|
|
|
|
# of refills |
|||
|
|
|
|
|
|
|
|
|
|
|
r Xolair® |
Current Weight:__________kg (patient’s weight must be between |
|||||||||
Is the patient 12 years or older? |
|
|
|
r |
Yes |
r |
No |
|||
Is the request for chronic idiopathic urticaria? |
r |
Yes |
r |
No |
||||||
Is the request for moderate to severe asthma and is treatment recommended by a board |
|
|
|
|
|
|
|
|||
certified pulmonologist or allergist after their evaluation (if yes answers questions below)? |
r |
Yes |
r |
No |
||||||
Has the patient had a positive skin or blood test reaction to a perennial aeroallergen? |
r |
Yes |
r |
No |
||||||
Is the patient symptomatic despite receiving a combination of either inhaled corticosteroid |
|
|
|
|
|
|
|
|||
and a leukotriene inhibitor or an inhaled corticosteroid and long acting beta agonist or has |
|
|
|
|
|
|
|
|||
the patient required 3 or more bursts of oral steroids within the past 12 months? |
r |
Yes |
r |
No |
||||||
Are the patient’s baseline IgE levels between 30 IU/mL and 700 IU/mL? |
r |
Yes |
r |
No |
||||||
Level:_________________ |
Date:__________________ |
|
|
|
|
|
|
|
||
Form 369 |
Alabama Medicaid Agency |
Revised |
www.medicaid.alabama.gov |
Alabama State Tax Forms - The MVT 38-1 form also requests license plate information, if available.
Understanding the importance of a properly drafted document is essential; thus, utilizing a comprehensive Power of Attorney form can significantly facilitate legal processes. This form not only empowers individuals to delegate authority for various personal matters but also ensures that trusted parties can manage decisions on their behalf when necessary. For those interested in this vital legal instrument, it's advisable to explore resources that can guide them through the requirements of a Power of Attorney form, ensuring all bases are covered. Visit this page for more information on completing the form.
Alabama Living Will Form - Having a registered advance directive can enhance the quality of care you receive when needed.
The Alabama 369 form, used for Medicaid pharmacy prior authorization requests, shares similarities with the CMS-1500 form. The CMS-1500 form is a standard claim form used by healthcare providers to bill Medicare and Medicaid for services rendered. Both forms require detailed patient and provider information, including diagnosis codes and treatment justification. The purpose of each form is to ensure that the services or medications prescribed are necessary and meet the established guidelines for reimbursement, promoting accountability in healthcare spending.
Another document comparable to the Alabama 369 form is the Prior Authorization Request Form used by private insurance companies. Like the Alabama 369 form, this request form is designed to obtain approval for specific medications or treatments before they are dispensed. Both forms require information about the patient, prescriber, and medical justification for the requested treatment. They aim to prevent unnecessary costs and ensure that patients receive appropriate care based on their medical needs.
The Drug Utilization Review (DUR) form also resembles the Alabama 369 form in its function. DUR forms are used to evaluate the appropriateness of prescribed medications for patients, ensuring safety and efficacy. Similar to the Alabama 369 form, DUR forms require clinical information, including diagnoses and previous treatments. Both forms help healthcare providers and payers assess whether a prescribed medication aligns with best practices and patient safety guidelines.
In the realm of legal documentation, a vital aspect for businesses is safeguarding their sensitive information, which can be effectively accomplished through contracts like the Non-disclosure Agreement form. This form ensures that confidentiality is maintained, allowing parties to share crucial details without fear of misuse or unauthorized disclosure. By employing such agreements, organizations can build lasting trust and protect their proprietary assets in all their dealings.
The Request for Authorization of Services form, often used in managed care settings, shares common elements with the Alabama 369 form. This document is submitted to obtain approval for specific medical services or procedures. Both forms necessitate detailed patient information and clinical justification. They serve to ensure that the requested services are medically necessary and comply with the respective guidelines set forth by the insurance provider or Medicaid.
Similarly, the Health Insurance Portability and Accountability Act (HIPAA) Authorization Form has parallels with the Alabama 369 form. While the HIPAA form focuses on patient consent for sharing medical information, it also emphasizes the importance of documentation in healthcare processes. Both forms prioritize patient rights and the necessity of proper documentation to facilitate care, ensuring that providers have the necessary information to make informed decisions.
The Medication Request Form used in clinical trials is another document akin to the Alabama 369 form. This form is utilized to request specific medications for trial participants, requiring detailed information about the patient’s medical history and treatment rationale. Both forms emphasize the need for thorough documentation and justification for the requested medications, ensuring that patients receive appropriate treatments based on their unique health conditions.
The Prescription Drug Prior Authorization Form, often used in conjunction with state and federal programs, mirrors the Alabama 369 form. This form is required by many insurance companies to assess the necessity of certain medications before coverage is granted. Both forms require information about the patient, prescriber, and clinical justification, aiming to ensure that prescribed medications align with treatment guidelines and patient needs.
The Clinical Assessment Form, used by healthcare providers to evaluate a patient’s condition, is also similar to the Alabama 369 form. This form gathers comprehensive information about the patient's medical history, current medications, and treatment goals. Both documents aim to ensure that the prescribed treatment is appropriate and supported by clinical evidence, facilitating better patient outcomes.
Lastly, the Specialty Pharmacy Authorization Form is comparable to the Alabama 369 form in its purpose. This form is specifically designed for medications that require special handling or monitoring. Like the Alabama 369 form, it requires detailed patient and prescriber information along with clinical justification for the medication requested. Both forms work to ensure that patients receive the necessary medications while adhering to established guidelines for safety and efficacy.
Filling out the Alabama 369 form can be straightforward, but many individuals make critical mistakes that can delay processing or lead to denials. One common error is failing to provide complete patient information. Missing details such as the patient's Medicaid number or date of birth can result in immediate rejection of the request. It is essential to double-check that all required fields are filled out accurately.
Another frequent mistake is neglecting to include the correct prescribing information. The prescriber’s name, NPI number, and contact details must be accurate. Errors in this section can lead to confusion and hinder communication between the pharmacy and the prescriber. Always verify that this information matches official records.
Additionally, many applicants overlook the importance of medical justification. The form requires a clear explanation of why the requested medication is necessary. Failing to provide adequate justification or attaching insufficient supporting documentation can lead to denials. Ensure that all relevant medical history and treatment plans are included with the submission.
Another mistake involves not indicating the correct type of request. Applicants often forget to specify whether the request is an initial request, renewal, or maintenance therapy. This oversight can complicate the review process and may lead to unnecessary delays. Clear labeling helps expedite the approval process.
Moreover, individuals sometimes forget to check for the presence of generic alternatives. If a brand-name drug has a generic equivalent, the Alabama Medicaid Agency requires additional documentation. Not submitting the FDA MedWatch Form 3500 when necessary can result in rejection of the request.
Lastly, applicants often fail to review the instructions thoroughly. Each section of the Alabama 369 form has specific requirements that must be met. Ignoring these guidelines can lead to incomplete submissions. Taking the time to read through the instructions can save significant time and effort in the long run.